Bi monthly exam Jan 16
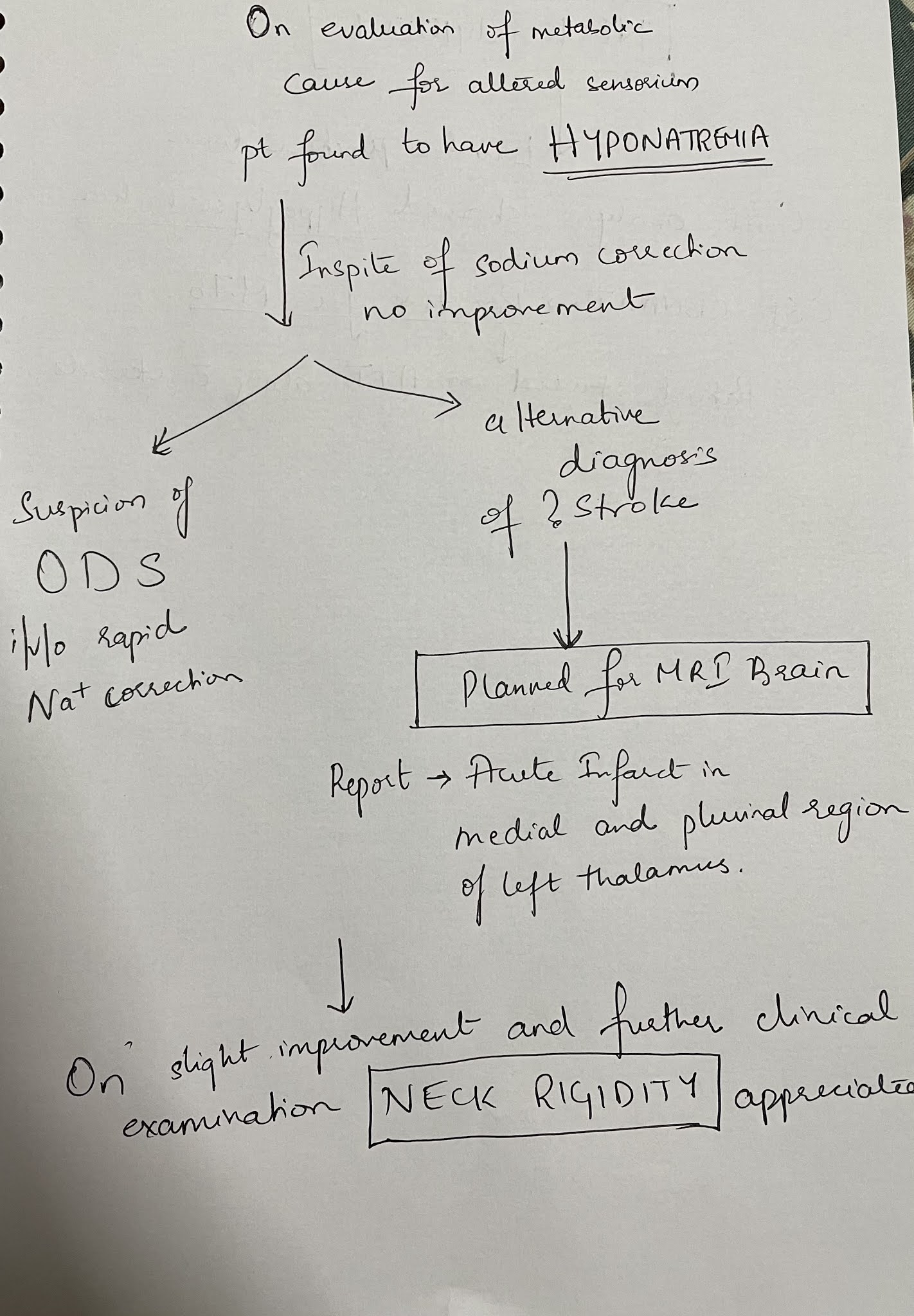
26 year old woman with complaints of altered sensorium somce 1 day,headache since 8 days,fever and vomitings since 4 days

‘’Two-month treatment with HCQ resulted in significant decrease in SLEDAI-2K (p < 0.001), anti-dsDNA (p < 0.001), IL-1β (p = 0.003), IL-6 (p < 0.001) and TNF-α (p < 0.001) and a significant increase in CH50 levels (p = 0.012). ‘’
Pooled analysis for incident nonvertebral fractures included nine trials with 1245 participants with low‐certainty evidence (downgraded for imprecision and serious risk of bias as a patient‐reported outcome). In this analysis 30/546 (or 55 per 1000) people experienced new nonvertebral fracture in the control group compared with 29/699 (or 42 per 1000; range 25 to 69) in the bisphosphonate group
Cardiovascular.
In a study that involved 19 normotensive individuals without diabetes, 17 hypertensive individuals without diabetes, and 6 hypertensive individuals with diabetes, Resnick et al. documented the lowest mean intracellular Mg concentration among the last group. Similarly, based on data from the Atherosclerosis Risk in Communities (ARIC) Study, a multicenter, prospective cohort study that lasted 4 to 7 yr and involved 13,922 middle-aged adults who were free of coronary heart disease at baseline, an inverse association between serum Mg and the risk for coronary heart disease was observed among men with diabetes
Diabetic Retinopathy.
The link between hypomagnesemia and diabetic retinopathy was reported in two cross-sectional studies that involved both “insulin-dependent” patients and patients with type 2 diabetes. Not only did patients with diabetes have lower serum Mg levels compared with their counterparts without diabetes, but also the serum Mg levels among the cohort with diabetes had an inverse correlation with the degree of retinopathy .
Foot Ulcerations.
Given the link between hypomagnesemia and risk factors for the development of diabetic foot ulcers (e.g., polyneuropathy, platelet dysfunction), Rodriguez-Moran and Guerrero-Romero (48) suggested that hypomagnesemia may be associated with an increased risk of diabetic foot ulcers. Indeed, they observed a higher incidence of hypomagnesemia among their patients with diabetic foot ulcers compared with those without the condition (93.9% of the 33 patients with diabetic foot ulcers compared with 73.1% of the 66 patients without diabetic foot ulcers; P = 0.02).
Nephropathy.
In a comparative study that involved 30 patients who had type 2 diabetes without microalbuminuria, 30 with microalbuminuria, and 30 with overt proteinuria, Corsonello et al. (49) observed a significant decrease in serum ionized Mg in both the microalbuminuria and overt proteinuria groups compared with the nonmicroalbuminuric group. Accordingly, in a recent retrospective study, an association between low serum Mg levels and a significantly faster rate of renal function deterioration in patients with type 2 diabetes was reported (7).
Others.
Finally, there also are data to suggest the association between hypomagnesemia and other diabetic complications, including dyslipidemia and neurologic abnormalities.Because hypomagnesemia has been linked to various micro- and macrovascular complications, a better understanding of Mg metabolism and efforts to minimize hypomagnesemia in the routine management of diabetes are warranted.
Source:



Comments
Post a Comment