Short case
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient - centered online learning portfolio and your valuable inputs on the comment box"
A 62 yr old female, home maker by occupation presented to OPD with the
Chief complaints of
-Shortness of breath on exertion since 5 days
-Bilateral lower limb swelling since 5 days
-Decreased urine output which was worsening since 5 days
The above chief complaints were gradually progressive from last one year and patient had debilitating effects from last one week.
HISTORY OF PRESENTING ILLNESS :
Patient was apparently asymptomatic 20 years back , was diagnosed to be diabetic incidentally on routine workup an an instance of fever and was started on oral hypoglycaemic agents on TAB.GLIMI2
1990 :
She underwent tubectomy
2002 :
Pt developed pain abdomen for which pt was admitted in hospital and undergone HYSTERECTOMY ?FIBROIDS .
2009:
Pt developed chest pain for which he was admitted in hospital and she was taken for primary PTCA.
On angiogram it was showing a double vessel disease (RCA+ LAD)
Since 2009 she had intermittent episodes of pain abdomen in epigastric region which was relieved on medication with PPI.
2012
Underwent cataract surgery in two eyes with 6 months interval
2016:
She had another episode of chest pain she was taken to hospital and was taken for primary PTCA to LAD ?stent thrombosis.
Around 2021 :
She developed bilateral pedal oedema associated with decreased urine output ,shortness of breath was diagnosed to be having a renal disease and was started on medication accordingly and continued to use OHA’s intermittently with insulin and stopped using because of poor compliance.
Pt had an episode of sweating, palpitations with slurring of speech and deviation of angle of mouth followed by unresponsiveness, her GRBS was 35mg/dl. MRI brain was done showing no structural lesions, and was diagnosed to be hypoglycemic seizure episode (sweating, slurred speech, deviation of mouth and unresponsiveness) and the symptoms reverted after correction of hypoglycaemia, this episode was attributed to the change in her dosage and timing of OHA’s.
She had similar history of developing pedal oedema on and off with decreased urine output and shortness of breath 5 months back. Patient was evaluated and was found to have anemia which was managed by systemic iron therapy.
From the past one month patient started experiencing, nausea, vomiting, loss of appetite and dyspepsia.
Presently admitted for similar complaints.
General examination:
Patient is conscious, coherent, co-operative, oriented to time, place and person.
No Icterus, Cyanosis, Lymphadenopathy,
Pallor ++
B/l pitting type Edema +
Vitals:
Bp: 100/70mmHg
PR: 96bpm
SpO2: 98%@RA
Temperature:98. 6°F
GRBS: 102 mg/dl
SYSTEMIC EXAMINATION :
CARDIOVASCULAR SYSTEM :
S1, S2 +, mid diastolic murmur in Tricuspid and mitral area.
Apex beat in 5th ICS on the MCL.
JVP normal.
RESPIRATORY SYSTEM :
Shape & symmetry of chest - Normal
Respiratory movements - Equal on both sides
BAE+
NVBS
Abdominal Examination
Soft, Non-tender
No organomegaly
Bowel sounds+
CNS :
Higher Mental Functions : intact
Cranial nerve Examination : no abnormality detected.
MOTOR SYSTEM
Right. Left
Bulk Normal Normal
Tone Right Left
Upper limb Normal Normal
Lower limb Normal Normal
✓Power
UL
Proximal 5/5 5/5
Distal 5/5 5/5
LL
Proximal 5/5 5/5
Distal 5/5 5/5
✓Reflexes
Superficial reflexes
Right Left
Plantar - -
Deep tendon reflexes
Right Left
Biceps 2+ 2+
Triceps 2+ 1+
Supinator 1+ Absent
Knee 2+ 2+
Ankle 1+ 1+
✓SENSORY SYSTEM
Right Left
Pain + +
Fine touch + +
Temperature + +
Vibration Intact Intact
Proprioception Intact Intact
Stereognosis Normal Normal
Gait - Normal
CEREBELLUM FUNCTIONS : Intact.
AUTONOMIC
No postural hypotension.
No urinary urgency, frequency, hesitancy.
No diaphoresis.




B/L pedal edema

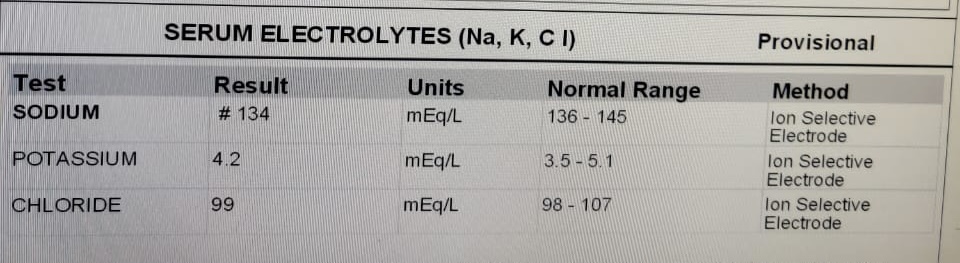
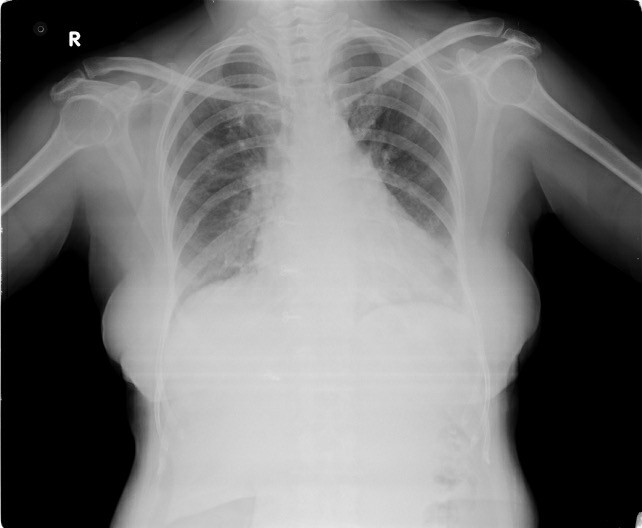
INVESTIGATIONS:






Chest xray -Pa view
ECG:


USG ABDOMEN :

Diagnosis:
ANEMIA SECONDARY TO CHRONIC KIDNEY DISEASE
? DIABETIC NEPHROPATHY
S/P:OLD CAD -PTCA +DES TO LAD (2009 ,2016)
WITH TYPE -2 DM SINCE 20 YEARS

Comments
Post a Comment