50 yr old male with Dilated cardiomyopathy secondary to alcohol
CHEIF COMPLAINTS:
A 50 year old male who is a daily wage worker came to the OPD with the cheif complaints of bilateral swelling in lower limbs which has extended till abdomen since 2 months and shortness of breathe ,decreased urine output and abdominal distension for the past 15 days .
HISTORY OF PRESENT ILLNESS:
Patient was apparently asymptomatic 3 years ago after which he visited a health care centre with complaints of diminished vision in his eyes where he was diagnosed with diabetes for which he is under medication with OHA's .patient does moderate work and gets adequate sleep daily .2 months ago one morning he noticed bilateral swelling in his feet which was insidious in onset and gradually progressive which he ignored and continued his routine for 5 days until he noticed the extension of swelling to his knees till the abdomen which did not subside after taking tablets for 10 days prescribed by doctor in Nakrekal .15 days ago he went to Nalgonda with same complaints of swelling now a/w decreased output and dribbling of urine for which he was catheterized with Foley's.He also complained of abdominal distension and SOB which is insidious in onset and gradually progressed from grade 3 to grade 4 a/w orthopnoea and Paroxysmal Nocturnal Dyspnea for which he was referred to this hospital.




PAST HISTORY:
Patient was diagnosed as diabetic when he went for eye checkup for diminished vision in both eyes 4 years ago and is receiving medication- OHA's
Pes cavus on right foot.
FAMILY HISTORY:
No similar complaints
PERSONAL HISTORY:
Appetite- normal
Diet- mixed
Bowel habits- regular
Bladder habits- oliguria
Sleep- adequate
Addictions- chronic alcoholic consumes 180ml/day
Chronic smoker smokes 10 cigarettes/day
Allergies- no allergies
GENERAL PHYSICAL EXAMINATION:
Patient is conscious coherent and cooperative
Pallor- no pallor
Icterus- present
Cyanosis- no cyanosis
Clubbing- no Clubbing
Generalized lymphadenopathy- no Generalized lymphadenopathy
Pedal edema- pitting edema in both the limbs extending till abdomen
Vitals:
Temperature- afebrile
Pulse rate
Rate-86bpm
Rhythm- regular
Volume- normal
Character- normal
Radioradial delay- no radioradial delay
Respiratory rate- 20cpm
Blood pressure- 124/84 mm Hg in right arm in supine position
SYSTEMIC EXAMINATION:
CARDIOVASCULAR SYSTEM:
INSPECTION:
Chest shape and symmetry- elliptical and bikaterally symmetrical
JVP : raised and prominent
Precordial examination:
A keloid at the mid line of chest.

No visible pulsations and engorged veins
Apical impulse - seen in the 6th intercostal lateral to mid clavicular line
https://youtube.com/shorts/8YolHDVDcgs?feature=share
https://youtube.com/shorts/RU5FovcchVU?feature=share
PALPATION:
inspectory findings confirmed
No tenderness and local rise of Temperature
Parasternal heaves- felt on left side
No precordial bulge
Apex beat - felt in the 6th intercostal space 2 inches from midclavicular line.
Thrills - absent
No other pulsations felt
No murmurs
PERCUSSION:
Heart borders: extended dullness on percussion to the lateral side.
AUSCULTATION:
HEART SOUNDS: S1 and S2 heard
S3 gallop is prominent in mitral area
RESPIRATORY SYSTEM :
Normal vesicular breathe sounds with thoracoabdominal type of breath movements. Bilateral air entry present
CENTRAL NERVOUS SYSTEM:
No focal neurological deficit
Higher motor functions normal
PER ABDOMEN:
Abdomen : distended soft and non tender
Umbilicus: everted

Liver and spleen are not palpable.
Bowel sounds : heard
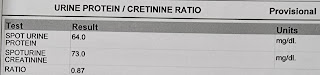
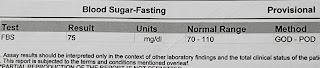
INVESTIGATIONS:
CHEST X RAY:

LIVER FUNCTION TEST:
Alkaline phosphatase- 210IU/L
Albumin- 3.0gm/dl
















Global akinetic , mild LUH(+) (102 cms)
Severe TR+ with PAH (60+20 = 80 mmHg)
Moderate MR+, mild AR+/PR+
Sclerotic AV no AS/MS
EF= 30%
Severe LV dysfunction(+)
Diastolic dysfunction (+)
Minimal PE(+)
IVC size (1.7cms) dilated
All chambers dilated
PROVISIONAL DIAGNOSIS:
DILATED CARDIOMYOPATHY SECONDARY TO HrfEF.
TREATMENT:
1.propped up Posture
2.Fluid restriction to <1.5Lt / day
3.Inj Lasix 40mg/IV/BD
4.Inj Human actrapid /SC (based on the grbs levels)
5.Inj thiamine 2amp in 100ml NS/IV/BD
6.Tab Ecospirin AV 75/20mg PO/OD
7.Strict Grbs monitoring 6th hourly
8.O2 inhalation (if spO2<92%)
9.Daily weight monitoring
10.I/O monitoring

Comments
Post a Comment